By 2026, the U.S. and Europe are seeing more drug shortages than ever before-not because of a single factory shutdown or a bad harvest, but because of a perfect storm of interconnected pressures. Insulin, antibiotics, cancer drugs, and even basic painkillers are vanishing from shelves, not temporarily, but for months at a time. The question isn't just why this is happening anymore. It's how bad it will get by 2030.
Why Drug Shortages Are Getting Worse
Drug shortages used to be about one plant going offline. Now, it’s about three continents failing to keep up at once. The global supply chain for active pharmaceutical ingredients (APIs) is still mostly tied to China and India. Together, they produce over 80% of the world’s raw drug components. But that’s not the whole story.
Climate disruptions are hitting agricultural regions where key raw materials grow. Droughts in southern India have cut the supply of plant-based precursors for painkillers like morphine. Floods in China’s Jiangsu province shut down API factories for months in 2024. These aren’t rare events anymore-they’re becoming seasonal.
At the same time, regulatory delays are piling up. The FDA and EMA are taking longer to approve new suppliers because they’re overwhelmed. A single change in a manufacturing process can take 18-24 months to clear. That’s too long when a drug is already running out.
The Numbers Don’t Lie
In 2023, the U.S. saw 298 drug shortages. In 2025, that number jumped to 417. The American Society of Health-System Pharmacists (ASHP) tracks this closely. Their data shows that 63% of shortages in 2025 were for injectable drugs-things hospitals can’t live without: antibiotics like vancomycin, chemotherapy agents like doxorubicin, and anesthetics like propofol.
By 2030, projections suggest the number of critical drug shortages could hit 600 per year. That’s not a guess. It’s based on modeling from the World Bank, the OECD, and the U.S. Department of Health and Human Services. Their models factor in population aging, rising chronic disease rates, and shrinking manufacturing capacity.
Here’s the kicker: global demand for essential medicines is expected to rise by 45% between 2025 and 2030. Meanwhile, the number of active API manufacturing facilities in the U.S. and EU has dropped by 18% since 2019. We’re asking more from fewer sources.
Who’s Most at Risk?
It’s not just hospitals. Rural clinics, nursing homes, and even pharmacies in low-income neighborhoods are hit hardest. A 2025 study in the Journal of the American Pharmacists Association found that patients in rural areas were 2.3 times more likely to go without a prescribed medication during a shortage than those in urban centers.
Why? Because urban hospitals can afford to pay 300% above list price to keep stock. Rural clinics can’t. They wait. And when they do, patients suffer. One case from Ohio in late 2024 involved a diabetic patient who ran out of insulin for 11 days because the local pharmacy couldn’t get a shipment. Her HbA1c spiked to 12.8%. She ended up in the ER.
Even in wealthy countries, access is becoming unequal. The same shortage that causes a delay in a big-city hospital can be life-threatening in a small town.
The Role of Geopolitics
Trade tensions aren’t just about tariffs. They’re about control. In 2024, India restricted exports of 12 key APIs to protect its domestic supply. China did the same with antibiotics. Suddenly, hospitals in Germany and Canada couldn’t get the raw materials they needed.
The World Economic Forum’s 2025 Future of Jobs Report points to this as a major driver of scarcity: geoeconomic fragmentation. Countries are pulling back, prioritizing their own populations, and cutting off global flows. It’s happening with energy, food, and now medicine.
Some companies are trying to respond. Pfizer and Novartis have started investing in small-scale API production in Eastern Europe. A new facility in Poland now supplies 15% of the EU’s metformin. But it’s not enough. These projects take 5-7 years to come online. We’re already behind.
What’s Being Done-and Why It’s Not Enough
The U.S. passed the Drug Supply Chain Security Act in 2013. It was supposed to prevent counterfeit drugs and improve traceability. It didn’t fix shortages. It just made the paperwork harder.
In 2025, the FDA launched the Medicine Shortage Prevention Initiative. It includes faster approval for backup suppliers and incentives for domestic production. But only 12 companies have applied so far. Why? Because building a new API plant costs $300 million. No private investor wants that risk unless they’re guaranteed 10-year contracts-and the government won’t offer them.
Meanwhile, the EU is trying to force bulk purchasing across member states. It sounds smart. But in practice, it’s creating new bottlenecks. When France and Germany both order 500,000 units of the same drug, suppliers can’t meet both demands. They pick one.
What Could Change by 2030
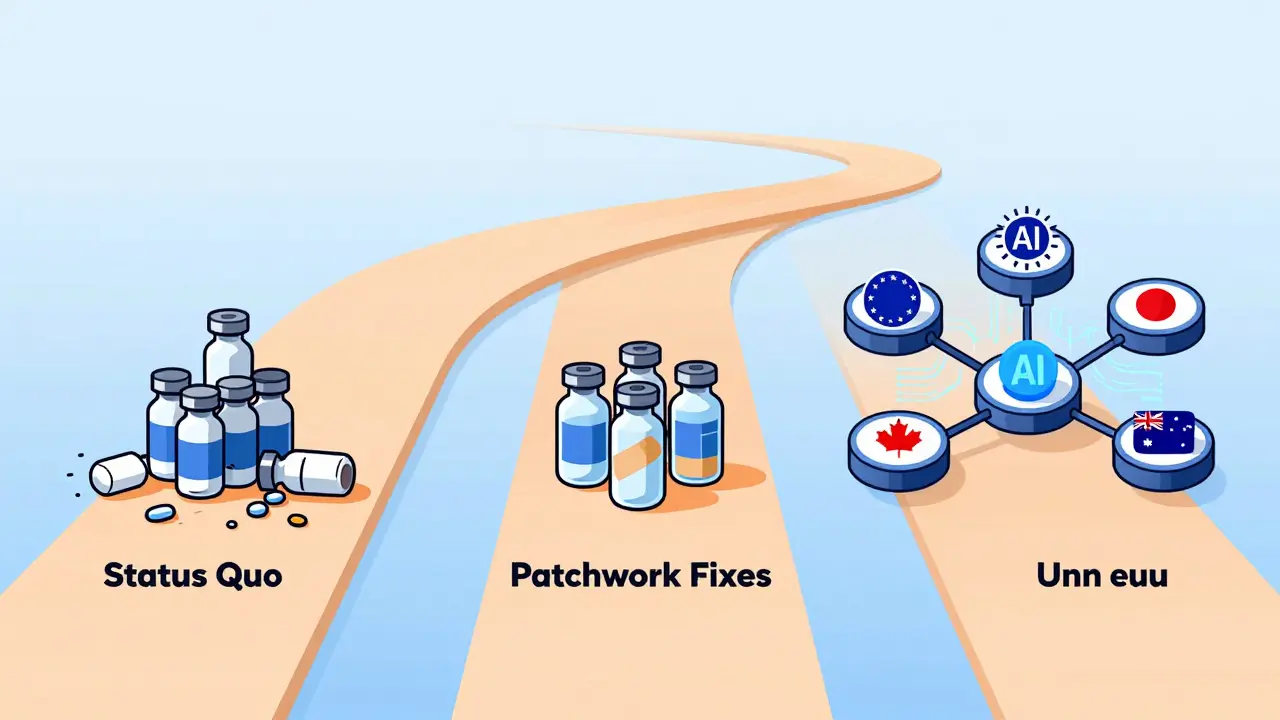
There are three paths forward-and only one leads to real stability.
- Path 1: Status Quo - Shortages keep getting worse. By 2030, 1 in 4 essential drugs will be unavailable for more than 30 days per year. Hospitals will ration. Patients will die.
- Path 2: Patchwork Fixes - Governments give subsidies to a few manufacturers. Shortages slow, but only for a handful of drugs. Most remain vulnerable. This is where we are now.
- Path 3: Systemic Shift - A global alliance forms: U.S., EU, Japan, Canada, and Australia agree to co-invest in a network of regional API hubs. Each hub serves 50 million people. They use AI to predict demand, share inventory in real time, and rotate production. This isn’t science fiction. The UK’s NHS is already testing a version of this with insulin and antibiotics.
The third path works. It’s been proven in pilot programs. But it requires trust. And political will. Neither is easy to come by.
What You Can Do (Even If You’re Not a Pharmacist)
You might think this is a problem for hospitals and policymakers. But it’s not. If you take a daily medication, you’re one shortage away from crisis.
- Ask your pharmacist: “Is this drug on shortage?” They’re required to tell you.
- Keep a 30-day backup supply if your medication is critical (like insulin, blood thinners, or seizure meds). Talk to your doctor about it.
- Support policies that fund domestic manufacturing. Vote for representatives who prioritize drug supply security.
- Don’t hoard. Stockpiling creates artificial shortages and hurts those who need it most.
The system is breaking. But it’s not broken yet. What happens next depends on who acts-and how fast.
Why are generic drugs more likely to be in shortage than brand-name drugs?
Generic drugs are made by multiple manufacturers, but they’re sold at low prices. Because profits are thin, companies often stop producing them when costs rise-like when raw materials get expensive or regulations change. Brand-name drugs have patents that protect pricing, so companies keep making them even if they’re costly. That’s why 80% of shortages are for generics.
Can AI really help predict drug shortages?
Yes. The NHS in the UK uses AI to track 120+ data points: weather patterns affecting crops, shipping delays from Asia, factory maintenance schedules, and even social media reports from pharmacists. Their system predicted a 2025 shortage of metformin three months in advance. That gave hospitals time to switch suppliers. Without it, 12,000 patients would’ve gone without.
Are there any drugs that are completely immune to shortages?
No drug is completely immune. But some are less vulnerable. Vaccines, for example, are often produced under government contracts with guaranteed purchases. Cancer drugs with few alternatives are also prioritized. Still, even these have faced delays-especially when raw materials come from regions hit by conflict or climate events.
How long does it take to start making a drug domestically?
At least 5 years. You need to build a facility, get FDA/EMA approval, train staff, and qualify every batch. Even with fast-tracking, it’s 3-4 years minimum. That’s why planning now is critical-waiting until a shortage hits means it’s already too late.
What’s the difference between a drug shortage and a supply delay?
A delay is temporary-days or weeks-usually due to weather or transport. A shortage lasts 30+ days and means there’s no available supply from any manufacturer. Shortages require switching to alternatives, which isn’t always safe. Delays just mean waiting. Shortages mean risking your health.

phyllis bourassa
March 6, 2026 AT 00:15Okay but let’s be real - we’re just waiting for the next pandemic-level collapse to happen, aren’t we? Insulin shortages? In 2025? In *America*? I’ve got a cousin who’s diabetic and she’s already rationing doses because her pharmacy runs out every other month. This isn’t a supply chain issue - it’s a moral failure.
And don’t even get me started on how rural folks are getting screwed. You think a nursing home in Nebraska can afford to pay 300% more for vancomycin? Nah. They just tell Grandma to tough it out until the next shipment ‘maybe’ comes. That’s not healthcare. That’s neglect with a clipboard.
Joe Prism
March 7, 2026 AT 15:15It’s not about manufacturing. It’s about incentives.
Profit drives production. No profit? No drug. Simple.
Bridget Verwey
March 9, 2026 AT 02:17Oh sweet baby Jesus. We’re doing a full-on performance art piece of societal collapse and calling it ‘pharmaceutical policy.’
Let me get this straight - we’ve got AI that can predict a metformin shortage three months out, but we won’t fund a single API plant because ‘it’s too risky’? Meanwhile, we drop $800 billion a year on defense. Where’s the priority?
Also - hoarding is bad. But so is pretending this is just a ‘supply issue.’ It’s a greed issue. And we’re all complicit.
Andrew Poulin
March 9, 2026 AT 12:06Stop the handwringing. Build the plants. Pay the workers. Fix the approvals.
That’s it. No more meetings. No more reports. Just do it.
Weston Potgieter
March 11, 2026 AT 08:09Everyone’s mad at China and India but nobody talks about how we outsourced everything because we were too lazy to pay for good manufacturing here
Also why are we still using 1980s regulatory systems for 2025 supply chains
And why does no one mention that 80% of shortages are generics because no one wants to make pennies on a pill
Also why are we surprised
Also also why are we surprised
Also also also why are we surprised
Vikas Verma
March 12, 2026 AT 12:24As an industry professional from India I can confirm the raw material disruptions are not isolated incidents but systemic vulnerabilities in agro-pharma ecosystems
Climate volatility has directly impacted alkaloid yields in southern states and we are witnessing a structural shift in API sourcing dynamics
Moreover regulatory harmonization remains fragmented and this is exacerbating lead times exponentially
Without coordinated multilateral investment in regional manufacturing clusters we are headed for a crisis of unprecedented scale
Sean Callahan
March 13, 2026 AT 06:49i just read this and i cant believe we let this happen
my mom takes blood thinners and last month she went 12 days without it because the pharmacy said ‘we’re out’
she almost had a stroke
why is this still a thing
why
why
why
Ferdinand Aton
March 13, 2026 AT 16:04What if the shortages are actually a feature not a bug?
Think about it - if everyone has access to everything, who profits? But if some people can’t get their meds? That’s when the black market thrives. And the black market? That’s where the real money is.
Just saying. 🤔
Adebayo Muhammad
March 14, 2026 AT 05:38Let’s not ignore the elephant in the room: The pharmaceutical-industrial complex is deliberately engineering scarcity to drive up prices, and then lobbying for ‘emergency’ subsidies to ‘save’ the system - while quietly acquiring smaller manufacturers and consolidating control.
It’s not climate, it’s not regulation - it’s monopolization.
And yes, I’ve seen the documents. I’ve seen the emails.
And no, I won’t name the names. But you know who you are.
Pranay Roy
March 15, 2026 AT 16:24China and India aren’t the problem - the real issue is that the FDA and EMA are controlled by shadowy biotech lobbies who want to keep small manufacturers out
They’ve been suppressing new API facilities for decades because they don’t want competition
And now they’re using climate as an excuse to justify their monopoly
Also - did you know that 70% of the raw materials for insulin come from genetically modified algae grown in secret labs in Texas?
It’s true. I read it on a forum.
Aaron Pace
March 17, 2026 AT 14:59we need to build more factories 🏭
and pay people more 💰
and stop being lazy 🥱
and vote for people who care 🗳️
and stop hoarding insulin 🚫💊
and also... maybe... just maybe...
we should all stop pretending this isn't happening 😔